REFERRAL TO THE DERMATOLOGISTDermatological conditions are very common. General practitioners see many skin problems in their daily practice. Most of these can be easily identified and treated by the GP themselves. Sometimes a referral to a dermatologist (skin specialist) is necessary. The GP will write a referral letter for this and contact a dermatologist in your area or at a hospital. If you have received a referral letter, your care is usually covered by your health insurance.Referral letter is requiredPlease note: new, stricter regulations were introduced in 2013 – without a referral, your visit to the dermatologist may not be covered. Therefore, always ask your GP or another referring physician for a referral. If you were referred for an emergency, you can also submit the referral later.DeductiblePay attention to your health insurance deductible. This deductible varies by policy, and you can set it yourself. A high deductible results in a lower monthly premium. However, if you have a high deductible, for example, €500, you must pay all bills yourself up to this amount. Only after that amount will your health insurer reimburse you.Care in kind policiesThere are very affordable policies that don't allow you to just see any dermatologist. With these health insurance policies, the insurer has made fee agreements with specific hospitals or dermatologists. You will therefore have to go to them. If you do want to see a different dermatologist, one with whom your insurer hasn't made an agreement, you may have to pay part of the bill yourself. This can sometimes be quite expensive. You will have to ask your insurer yourself whether your in-kind health insurance provider has a contract with a specific hospital. Your general practitioner doesn't have this information. It's impossible for a general practitioner to keep track of the price agreements the health insurers have made with all those different specialists.HOW MUCH DOES A VISIT TO THE DERMATOLOGIST COST?This question used to be very easy to answer because there were fixed rates. Nowadays, there are very complex reimbursement rules that were created because politicians and health insurers wanted market forces in healthcare . This has created complete chaos. No one knows what a treatment costs anymore. Administration has become very labor-intensive. Hospitals and health insurers have had to hire a lot of extra staff to manage healthcare administration according to the new rules. There's a significant backlog in administration, and many mistakes are made. And it's not working: healthcare costs haven't decreased since the introduction of market forces in healthcare, but have actually increased. Fixed rates for treatments are no longer used, but rather " care products " purchased by health insurers. Prices are negotiated. Therefore, a treatment is more or less expensive in one hospital than in another. The amounts paid by different health insurers for the same treatment in the same hospital are also not the same. Because the price agreements are also kept secret by hospitals and health insurers, it's no longer possible for the average patient to find out what a referral to a dermatologist costs.
Before the introduction of market forces in healthcare, a visit to a dermatologist didn't cost much, just a few tens of euros. Now it can cost hundreds of euros. This is due to the new funding system, called DBC ( diagnosis-treatment combination ). These are average prices for a specific condition. However, the prices are set so that the treatment should roughly cover the costs of the entire care.Hospital. This means that all sorts of fictitious amounts are included in the invoice (overhead costs). For example, a percentage is charged for anesthesia even though you've never been under it. A percentage is charged for a pathological examination of the skin even though this examination has never been performed. All costs incurred by the entire hospital, including the building costs, rent, heating, all managers, financial administration, the ward, the intensive care unit, and so on, are included in the invoice. That's why such absurdly high bills are issued for simple treatments. Most patients don't see these bills because they go straight to their health insurers. Those who are uninsured or poorly insured will see them and will be shocked. Medical specialists often receive calls from angry patients complaining about the high bill and the amounts listed for things that weren't done. Understandable, but not justified: the medical specialists didn't invent this strange system. Hopefully, this brief explanation has made it a little clearer how the DBC system works.
Some hospitals publish " passer-by price lists ." These are the amounts charged for treatments for patients who don't have health insurance (think tourists) or whose insurer doesn't have a contract with the hospital. These lists are long and confusing, but sometimes you can look them up for a specific treatment. The amounts listed provide a general idea. The final price can differ by 30-50% from what's listed on the outpatient price list. And then you also need to know the exact code for the treatment.
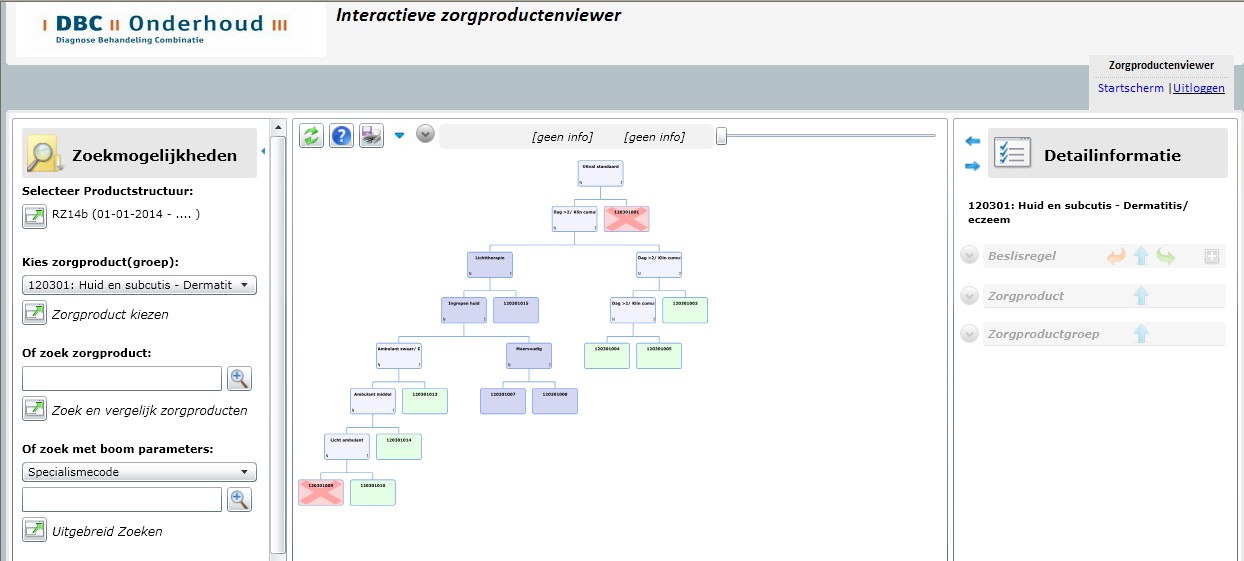
For example, on the outpatient price list for the AMC (AMC) 2013 , which can be found online, under declaration code 15D627 and care product code 120301014, one can find that a treatment or examination at the AMC's dermatology outpatient clinic for skin inflammation or eczema costs €411.25. Of this, €89.28 goes to the dermatologist, and the remaining €321.97 goes to the hospital for overhead costs. But there's another one, called declaration code 15C618, healthcare product code 120301010, description: outpatient clinic consultation for skin inflammation or eczema, which costs €149.96 (€43.93 for the dermatologist, €106.03 for the hospital). Which one is it? That's not clear from such a list. An even more complicated system, strangely enough called DOT (DBC on the way to transparency), determines which healthcare product code it will be.HOW MUCH DOES A TREATMENT BY A DERMATOLOGIST COST?As you'll understand from the previous story, it's become very difficult to say what a treatment costs. You can safely assume your dermatologist doesn't know either. The DBC system was already quite complex, but now it's been replaced by a new system called the DOT system , which is even less transparent. The hospital automation system records your outpatient visit. If the dermatologist performs a treatment, such as removing a mole, this is registered as a procedure. If you return after a week to have the stitches removed, another visit is registered. All these events (two visits and a treatment) are automatically submitted by the hospital software to a health insurer's software package called " the grouper ." This is a very large decision tree with many subpaths. The events are entered, and a care product code is generated, a number that corresponds to a specific care product. The number of visits, the number of procedures, and the nature of the procedures determine the final care product and therefore the rate. This rate is then negotiated between the health insurer and the hospital, so it remains unclear exactly what a treatment costs.
WHAT IS NO LONGER REIMBURSEED?Bath oil and skin care cosmeticsThese were the first products to be removed from the product line, years ago. Patients with atopic eczema, in particular, suffer from this, as they need to keep their skin constantly moisturized due to a compromised skin barrier. If they don't, the eczema worsens, requiring more intensive (and expensive) therapy to get it under control.Antibacterial productsProducts such as Betadine iodine scrub, Hibiscrub, iodine ointment, etc., are no longer covered. Health insurers consider these to be standard home care products, just like shampoo, soap, deodorant, bandages, etc. They're part of the general pharmacy.Anti-fungal productsProducts like Daktarin cream, dusting powder, and other antifungal preparations are no longer covered by insurance. These are commonly used products (also not very expensive) that are also available over the counter.Products against parasitesProducts to treat head lice and scabies are also no longer covered.
Over-the-counter products:
Many products available without a prescription (over-the-counter products) are no longer covered. For example, cold sore creams, antifungal creams, etc.Plasters and bandagesBandages are no longer reimbursed unless they must be prescribed for a longer period, such as for chronic wounds and serious wounds. In that case, they are reimbursed, provided the treating physician writes a prescription and completes a bandage authorization form .Bandages for atopic eczemaFor children and older patients with atopic eczema, bandage packs (scratch packs) are available. These are often made of silk, sometimes woven with silver thread, and are very expensive. An adult shirt can cost as much as €275. As of 2014, many insurers no longer cover these packs for adults, but they do cover them for babies and toddlers.Elastic stockingsSome insurers still reimburse genuine, custom-made therapeutic elastic stockings (of a certain compression class) if they are prescribed for poorly functioning veins or lymphatic vessels. Often, only one pair per year. If the same stockings are used as a follow-up treatment for varicose vein removal, reimbursement is no longer possible. Simpler stockings, ready-made stockings, and stockings with lower compression classes are also usually no longer covered. Furthermore, it now depends on the package you choose with your health insurer. Sometimes stockings are not included in basic insurance, but are included in supplementary insurance. Read your policy conditions carefully and contact your health insurer if necessary.Pay extraSome medications are partially reimbursed. Your pharmacist can tell you if you need to pay a supplement and how much. There's also a website run by health insurers, the pharmacotherapeutic compass , and www.medicijnkosten.nl, where you can look up the cost of a medication, whether you need to pay a supplement, and if so, how much. Here too, there are health insurance policies that don't require you to pay a supplement for certain medications.Diane 35The Diane-35 pill is prescribed by dermatologists for severe acne and excessive hair growth (hirsutism), but can also be used as a regular contraceptive pill. The pill was previously covered by insurance. This policy was abused (used as a regular contraceptive pill when it wasn't actually intended for that purpose). Effective February 1, 2014, the Diane pill is no longer covered by insurance.Benign bumps (benign tumors, DBC code 03)The removal of benign skin conditions (benign skin tumors), such as seborrheic keratosis, is no longer covered by insurance. This is considered cosmetic care.
This sometimes leads to unusual situations: a skin tumor needs to be removed because the dermatologist suspects a malignant tumor (skin cancer). The tumor is then examined by a pathologist. If the pathologist then diagnoses it as benign, the patient is initially relieved. However, if the dermatologist subsequently changes the diagnosis to benign, the patient has to pay the bill themselves. Benign tumors are not covered by insurance. According to health insurers, the dermatologist should have requested authorization in advance. However, the treatment takes weeks, and they are usually rejected. This is not possible; if a malignant tumor is suspected, it is always removed as quickly as possible.Vascular abnormalities (vascular lesions, DBC code 25)The treatment of vascular lesions (vascular abnormalities) such as hemangiomas (blood fins), couperose, and port-wine stains is no longer reimbursed unless authorization is given.Pigment disorders (DBC code 16)Pigmentation disorders, such as dark skin discoloration, but also discolorations like vitiligo, can be treated, for example, with laser. This is no longer covered by standard coverage, although sometimes it is with authorization.
For these three categories, the health insurer may, in some cases, approve the treatment if it concerns cosmetically very disturbing abnormalities, for example, on the face. Prior authorization (authorization) must be requested.
It is, of course, possible to remove these types of abnormalities that fall under uninsured care , but you should be aware that you will have to pay for the treatment yourself and that the costs can be high due to the calculation system of the DBC system.
Some dermatologists have found a solution in their hospitals or practices to perform these treatments. They charge separate, lower rates for uninsured care. Payment is often made in cash, just like at the dentist. ATMs are being purchased and agreements are being made with the hospital about how the extra revenue will be used. There are also dermatologists who completely stop performing treatments that are no longer reimbursed, and some dermatologists still perform them if they don't take too much time but simply stop charging for them. At university hospitals, treatments that are no longer reimbursed are often still performed: these are teaching hospitals, and it's important that resident physicians in dermatology training learn the profession properly, including procedures such as removing age-related warts and varicose veins.Varicose veinsThe treatment of small varicose veins with sclerotherapy (injection) is no longer covered by insurance. The treatment of large varicose veins with the Muller procedure and the treatment of large saphenous and parval veins with endovascular techniques are still covered.BotoxBotox is used in the cosmetics industry to eliminate wrinkles and crow's feet. But it was also used to treat hyperhidrosis (sweaty hands and armpits). This is an unpleasant condition, a bothersome skin disease, and in the past, Botox treatment was rightly covered by insurance. However, in 2012, the reimbursement rate was significantly reduced. The reimbursement the hospital receives for treating hyperhidrosis with Botox is much lower than the cost of the medication. This means that departments that use this treatment lose thousands of euros annually. For this reason, most dermatologists have stopped using it.Light therapyLight therapy is used for several skin conditions, particularly eczema and psoriasis, but also for other rare skin conditions. Previously, it was covered for all indications. However, since the introduction of the DBC system, some health insurers only reimburse it for eczema and psoriasis, and no longer for other rare skin conditions. The second change is that it also depends on the insurance package. With some affordable health insurance plans, light therapy is no longer included in the basic package, but only in the supplementary insurance.Light therapy at homeHome light therapy is considered a luxury by health insurers, but for some patients, it was a godsend. Until 2012, home light therapy was simply reimbursed by health insurers. In 2012, the policy changed: the bill for home light therapy was sent to the hospital. Hospitals could then reclaim this amount from their health insurers. In 2013, the reimbursement for home light therapy was drastically reduced to well below the cost price charged by providers to the departments. At the same time, due to budget cuts, many hospitals found that reimbursement for light therapy was not passed on to the departments, even though they were still required to pay the bills. As a result, departments had to pay tens of thousands of euros for home light therapy. Therefore, most departments and dermatologists stopped offering home light therapy. Patients with insurance can still receive light therapy at the outpatient clinic.Expensive medicinesPatients with psoriasis and other rarer skin conditions such as hidradenitis suppurativa, sarcoidosis, and pyoderma gangrenosum sometimes use expensive medications (biologics) called TNF inhibitors. These medications cost between €15,000 and €30,000 per year. Initially, these new medications were not reimbursed at all. Some hospitals had a budget to treat a few patients, but most did not. Between 2008 and 2012, these expensive medications were simply reimbursed by health insurers. In 2012, the regulations were changed: the costs were once again covered by the hospitals. Hospitals also received a larger budget to cover these costs. The minister promised that this budget would continue to be sufficient to treat these patients. However, in 2013, significant cuts to healthcare were implemented. Hospital care was rebudgeted, and individual departments were also rebudgeted. This means that patient numbers are no longer possible, and in some cases, departments are instructed by management to prescribe less expensive medications. Consequently, patients who are medically eligible for TNF inhibitor treatment will no longer be able to receive it in 2014 due to insufficient funding.Budget onThe ministry now seems to have realized that market forces in healthcare are completely dysfunctional: they are increasingly working with budgets again, and caps (2.5%) are being set on healthcare cost increases. Many hospitals have already abandoned market forces in healthcare and are simply using budgets, just like before. For example, they have agreed on a total amount with several major health insurers and must adhere to that hospital budget. Departments have also been given budgets to adhere to. They are not allowed to perform more treatments than agreed upon. This results in some departments being unable to perform certain treatments (such as knee and hip surgeries) at the end of the year, sometimes as early as November, because their budget has run out. December is therefore a bad month for hospitals: no more surgeries, little to do, but salaries still have to be paid. January is also a bad month: the increase in deductibles is effective, and patients are postponing doctor visits as long as possible. As a result, outpatient clinics are also quiet in January.Late billsHospital administrations are often behind in sending invoices. A delay of 1.5 years and even two years is common. Many errors are also made in registering the DBC. Only when everything is entered correctly into the computer does the system generate the correct data that can be presented to the grouper. The wrong treatment for the wrong diagnosis results in an error. Forgetting to enter the diagnosis or a procedure also results in an error. All these errors must be corrected manually. Additional staff has been hired for this purpose, but backlogs still exist. Many DBCs cannot be salvaged due to a lack of clarity about what has been done. These DBCs are then not invoiced. Invoices submitted too late (more than two years) are also not invoiced. This results in a significant loss for hospitals. The late invoices are also disruptive to the health insurers' operations (they do not provide a clear picture of the costs). And they are disruptive to patients, who sometimes receive an invoice after two years.Complications arose and now I have a higher billThis is an undesirable side effect of the system. Complications unfortunately do occur occasionally, which is unavoidable. When surgery is performed on the skin, wound infection, postoperative bleeding, or stitches can burst can occur. This often means a return trip to the hospital, multiple visits, and extra checkups. The DOT system automatically generates a higher bill at some point with more visits. This is annoying, but an unavoidable consequence of the automated system.WHERE CAN I GO WITH MY QUESTIONS ABOUT COMPENSATION ISSUES?As you'll understand after reading this brochure, reimbursement regulations have become so complex that medical specialists, including dermatologists, have lost track and can no longer answer the simple question: "What does a treatment cost?"
Sometimes, hospital administration can provide an answer. They do need a general idea of the treatment involved and can then run a simulation in the grouper on the health insurer's website to determine the care product code. However, hospital administrations are overloaded, and not all hospitals can offer this service anymore.
It's best to direct your questions to your health insurer. The health insurers devised the system, together with officials from the Ministry of Health, Welfare and Sport. They know best how it works.
After reading this brochure, you'll hopefully understand how complex healthcare administration has become. The new system sometimes causes anger and frustration, not only among patients but especially among the treating physicians, who spend a great deal of time on the complex administration. Valuable time they would rather have spent treating patients than registering incomprehensible healthcare products. It's also frustrating that all sorts of useful treatments are no longer reimbursed.
However, there's little point in directing this anger at doctors and hospitals: the Ministry of Health, Welfare and Sport and health insurers are responsible for these developments, and only through political channels can they influence this process. |